Despite much progress in lung cancer over the last decade, lung cancer is the most frequent cause of cancer death.
Globally, 1.8 million patients are diagnosed with lung cancer, while in the U.S., more than 220,000 new cases are diagnosed per year. To ensure the best quality care for lung cancer worldwide, it’s critical that patients are diagnosed and treated correctly. The IASLC, as the only global organization dedicated solely to the study of lung cancer and other thoracic malignancies, is in a unique position to facilitate the improvement of lung cancer care worldwide through education and research, and the development of standardized guidelines for detection, screening, and treatment.
The IASLC staging system is a well-validated and accurate system that has led to the development of several accompanying guidelines and educational materials. The IASLC Staging Manual in Thoracic Oncology is one such guideline and reports on the latest revisions of the tumor, node and metastasis (TNM) classifications of thoracic malignancies; namely, lung cancer, malignant pleural mesothelioma, carcinoma of the esophagus and of the esophago-gastric junction and thymic epithelial tumors.
Proper staging of lung cancer and other thoracic malignancies accurately is important for making treatment decisions and ensures the best standardized care for patients worldwide.
The history of the staging system
The IASLC established an international Staging Committee in 1997, now known as the Staging and Prognostic Factors Committee (SPFC). The IASLC SPFC collects and combines lung cancer data sets to inform changes to the lung cancer TNM staging system with worldwide representation including all treatment modalities.
The data sets include a large amount of data regarding the size of tumors, lymph node status, and metastasis. This data provided the basis for staging recommendations that were adopted by the Union for International Cancer Control (UICC) and the American Joint Committee on Cancer (AJCC). Before the IASLC Staging Project, data collected for staging of lung cancer came from a smaller group of patients, almost exclusively based in the U.S. and was based on about 6,000 patients.
The IASLC Staging and Prognostic Factors Committee (SPFC) proposed revisions to the lung cancer staging system for the 8th edition of the TNM Classification of Malignant Tumours. The Union for International Cancer Control (UICC) and the American Joint Committee on Cancer (AJCC) accepted these revisions, and the 8th edition of the TNM Classification was implemented in January 2017. In the United States and most of the world, implementation was delayed until January 2018; now, the new edition has been enacted worldwide.
Updating the staging system—impact on clinical practice
The new database, which informs the Eighth Edition of the TNM Classification of Lung Cancer (The IASLC added our data beginning with the Seventh Edition), consists of 94,708 eligible patients diagnosed around the world from 1999-2010. The objective was to further explore and analyze the impact on prognosis of tumor size and of the different T descriptors; the prognostic significance of tumor burden in hilar and mediastinal lymph nodes; and the confirmation of the revised M1 categories (M1a and M1b) of the seventh edition of the classification along with the prognostic impact of number and anatomic location of metastases.
Staging is a tumor classification system that, in principle, reflects the anatomical extent of the tumor based on the extent of the primary tumor (T), the nodal spread (N) and the distant metastases (M). Revisions from the 7th to 8th edition were made to achieve refined prognostic capabilities and to help clinicians stratify tumors/ patients based on expected prognosis. Treatment modalities are very much dependent on stages of the disease. Therefore, a uniform staging system is important for determining the best treatment modality for the individual patient. It is also important for comparisons of treatment results from clinical trials.
The second edition of the IASLC Staging Manual in Thoracic Oncology includes:
- Information on the four above-mentioned neoplasms, instead of the first edition’s sole focus on lung cancer and mesothelioma.
- Besides the chapters describing the basic TNM classifications of the four thoracic malignancies, there are chapters on the history of the TNM classifications of the four tumors that give a lot of background information on the development of their staging systems.
- There are original chapters on the new recommendations proposed by the IASLC for classifying lung cancers presenting with multiple lesions, for measuring tumor size and for coding the newly described adenocarcinoma in situ and minimally invasive adenocarcinoma, as well as on prognostic factors.
- There are color atlases graphically describing the TNM classifications of the four thoracic malignancies.
- Additional chapters assist in the classification of tumors with characteristics that do not fit in the present official descriptors.
Differences in the TNM Classification of Lung Cancer
The main differences between 7th and 8th editions are the following:
T Descriptors
In the T component of lung cancer, the T1 category was divided into three subcategories (T1a-T1c) according to 1-cm cutoff points of the greatest dimension. The T2 category now includes tumors larger than 3 cm but no more than 5 cm and was divided into T2a and T2b according to 1-cm cutoff points. Tumors larger than 5 cm, but no more than 7 cm were classified as T3, and tumors larger than 7 cm were classified as T4. Adenocarcinoma in situ (Tis(AIS)): tumors without a solid part on CT image or a pathologic invasive part) and minimally invasive adenocarcinoma (T1mi: tumors with a solid part of < 0.5cm on CT image or a pathologic invasive part of < 0.5 cm) were introduced. Sub-solid tumors 3 cm or less in the greatest dimension were recommended to be classified according to the size of the solid part on CT image or the pathologic invasive part. Involvement of main bronchus without carina was categorized as T2 regardless of distance to the carina. Total atelectasis or obstructive pneumonitis were downgraded from T3 to T2. Invasion of the diaphragm was upgraded from T3 to T4.
N Descriptors
The N component had no changes. However, analyses of the IASLC database revealed prognostic implications of the number of involved lymph nodes and of involved nodal stations. Exploratory analyses of survival showed that N1a (involvement of a single N1 nodal station) had better prognosis than N1b (involvement of multiple N1 nodal stations). N2a1 (involvement of a single N2 nodal station without N1 involvement) had a similar prognosis to N1b. N2a2 (involvement of a single N2 nodal station with N1 involvement) was correlated with a worse prognosis than N2a1 but a better prognosis than N2b (involvement of multiple N2 nodal stations).
M Descriptors
M1 categories were refined based on the number of the extrathoracic metastases. Single extrathoracic metastasis was categorized as M1b, and multiple extrathoracic metastases were categorized as M1c. M1a has not changed from the 7th edition, which included metastasis restricted to the thoracic cavity. Prognosis of M1a and M1b diseases were similar; however, due to the difference of anatomic extension of the tumor, M1a and M1b were categorized as different entities.
Tools and teaching aids to help clinicians worldwide
The IASLC offers a wealth of resources to help doctors and nurses worldwide stage lung cancer, including a Staging Manual in Thoracic Oncology, a Staging Handbook in Thoracic Oncology, a staging app, laminated staging cards and posters, a collection of peer-reviewed scientific articles, and a comprehensive website. These tools can assist with implementation of the protocol in routine daily care.
Finally, the IASLC Staging Articles contain the science behind the revisions introduced in the 8th edition of the TNM classification. These articles have to be read thoroughly because they provide all the necessary information on the database used for the revision, the methodology applied, the results of the numerous analyses and their interpretation. Any doubt that one may have reading the core information included in the laminates, posters and apps will be solved by reading the landmark paper (ref. Goldstraw P, Chansky K, Crowley J, et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol 2016;11:39-51.)
While the 8th Edition of the international staging system was recently published, the IASLC is currently working on the 9th Edition, which will include molecular characteristics added to the TNM system. Given the rapid progress in the understanding of lung cancer, it’s critical that our staging system keep up. Small changes in the precision of diagnosing and treating lung cancer can make large changes in a patient’s outcome.
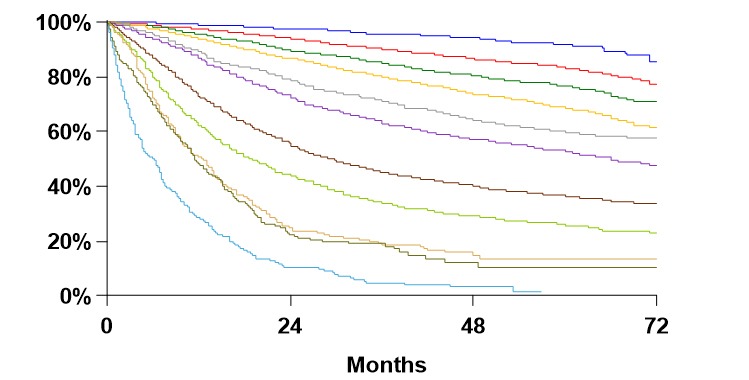
Overall Survival by Clinical Stage

Future projects
The IASLC is a multidisciplinary organization that includes surgeons, medical oncologists, radiation oncologists, pulmonologists, radiologists, pathologists, epidemiologists, basic research scientists, nurses, allied health professionals, advocates, caregivers and patients involved in lung cancer prevention and management.
Given the rapid progress in the understanding of lung cancer, it’s critical that our staging system keep up. Small changes in the precision of diagnosing and treating lung cancer can make large changes in a patient’s outcome.
The organization has grown significantly from 3,000 (2013) to about 8,000 members in >100 countries. Data from survival curves clearly shows that the earlier lung cancer patients are diagnosed, the better their outcomes. Thus, lung cancer screening and prevention efforts have high priority in IASLC. The IASLC is working on a global database for screening lung cancer patients more effectively and efficiently, hopefully helping the field take another large step toward the goal of making lung cancer a curable disease.
The IASLC is, of course, also involved in developing other educational and research activities and recently published CAP/IASLC/AMP guidelines for molecular testing of patients with lung cancer (ref. Lindeman NI, Cagle PT, Aisner DL, et al. Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment With Targeted Tyrosine Kinase Inhibitors: Guideline From the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology. J Thorac Oncol. 2018;13(3):323-358.)










