
The Association of American Cancer Institutes is designing two programs to address systemic underrepresentation of racial and ethnic minority physicians and scientists in leadership positions in oncology.

The two-year initiative is led by Caryn Lerman, AACI president and director of the USC Norris Comprehensive Cancer Center.
“The problem we are trying to solve with this initiative is the disconnect between the capacity and diversity of the current cancer center workforce and the needs of our increasingly complex cancer centers,” Lerman said at the virtual AACI meeting Oct. 20.
The leadership development programs will also be fulfilling an unmet need—an overwhelming proportion of cancer centers, up to 7 in 10, don’t offer formal leadership development programs, according to a recent AACI survey of 59 member cancer centers.
“Closing this gap requires many factors, including but not limited to building a diverse pipeline from both within and outside of the center, implementing deliberate and tailored leadership development to build the skills necessary to succeed in a complex cancer center environment, and ensuring that our centers provide comprehensive onboarding and mentoring for new and emerging cancer center leaders,” Lerman said.
Lerman’s initiative is the latest in a series of high-profile efforts in oncology to take meaningful steps toward increasing diversity in the workforce, improving access for minority patients, and reducing cancer disparities (The Cancer Letter, Health Equity, 2021).
The demographic results of the fall 2021 AACI survey mirror trends identified in a 2020 survey co nducted by The Cancer Letter in partnership with AACI, which found an urgent need for more diversity in leadership of North American academic cancer centers (The Cancer Letter, Oct. 9, 2020).
An independent study by Memorial Sloan Kettering Cancer Center researchers, who reached similar conclusions, found that racial and ethnic minorities that are underrepresented in medicine have even lower representation in leadership of NCI-designated cancer centers (The Cancer Letter, June 25, 2021).
The fall 2021 AACI survey, conducted by Lerman and her steering committee, found:
- The vast majority of cancer center directors (76.3%) and deputy directors (85.1%) are non-Hispanic white.
- Women make up only 14% of cancer center directors and 28% of deputy directors.
- About three quarters of cancer center associate directors (73.1%) and research program leaders (76.6%) are non-Hispanic white.
- There is greater gender parity among associate directors (44% women) and research program leaders (40% women).
“Considering our data, you see that even at the research program leader level in the cancer centers, the associate directors level, if we started there, we’d still be working with a talent pool that’s not especially diverse, as shown by the AACI data. So, it’s starting earlier,” Lerman said. “I would say, starting early, mining the talent pool among your members, looking for people with motivation, emotional intelligence, and just that ambition. And so, start at the beginning.
“There’s a lot of interest in these programs among faculty. The problem is then people go through this leadership development training, they get very excited, and then, because the current leaders—there’s no succession plans, often, there’s no term limits for certain roles—you have this excitement that you’ve generated, you don’t have the open positions for people to move up the food chain, and then they end up leaving,” Lerman said. “You have to actually create opportunities for leadership roles to move people into.
We’re not just saying, ‘In Philadelphia County, here’s the issue,’ but ‘In 400 counties across the United States, here’s an issue,’ becomes a much more empowering message.
Karen Knudsen
AACI, a professional organization for cancer center directors and leaders in North America, is the right vehicle for a leadership initiative like this, said Karen Knudsen, immediate past president of AACI and CEO of the American Cancer Society. Executive coaching and engagement can help young leaders get involved in each institution’s Cancer Center Support Grant process to obtain or renew NCI designation.
“AACI always provides training on CCSG and what’s new with NCI rules,” Knudsen said at the virtual meeting. “So, hopefully that’s a part of it. I see this as something for which the demand will only continue, not end in two years. This is certainly a developing business case for an incredible organization to take on what is a major gap in developing new leaders and do something about it.”
NCI, too, is refocusing its programs to ensure that the institute is looking at its entire portfolio “through a lens of health equity.”
“We all share responsibility to change this in whatever way we can and to bake health equity into sort of everything we do,” NCI Director Ned Sharpless said during his Calabresi Memorial Lecture at Yale Cancer Center Nov. 2. “Let’s build a reality in which your location, or your race, or your education doesn’t predict the outcome of your disease.”
A recent analysis of NCI’s workforce and grant recipients shows that Black and Hispanic scientists are dramatically underrepresented across key metrics, both intramural and extramural (The Cancer Letter, July 2, 2021).
“We’ve really redoubled our efforts to make headway against the problem of underrepresentation within the cancer research workforce,” Sharpless said.
NCI has deployed two programs—CURE and FIRST—to improve representation in the oncology workforce. The institute has also doubled its budget for health disparities-related research and training since 2015.
“Socioeconomic status alone can’t really capture what’s going on here. We need more sophisticated approaches to understand this interaction between rurality and poverty, particularly through time. A key for cancer disparities is to stop single-variable analyses and start working on these populations in their totality, with all their complexity.”
A story about Sharpless’s Calabresi Lecture appears here.
Lerman’s vision will dovetail with Knudsen’s ongoing 2020-2021 AACI presidential initiative to reduce cancer disparities across North America and collate best practices (The Cancer Letter, Oct. 16, 2020). To achieve that, Knudsen’s initiative is:
- Identifying cancer disparities in each center’s catchment area,
- Discovering currently implemented strategies for reducing disparities and opportunities for improvement, and
- Delivering an action plan for broader advocacy across the oncology community.
To date, 102 AACI member cancer centers have been surveyed. Of that number, catchment area and disparities data from 89 institutions have been analyzed and mapped.
“We did it by ZIP code, by county, and that’s how we overlapped the data as well with the population density, with incidence and with mortality. I credit our advisory group of leaders of AACI centers who helped us sort that through,” Knudsen said.”So, everything was funneled down to the county level.
“That’s why I went back out to the centers to say, here’s what we think you said using counties as a unit, so let us know if that’s right. So, if a county was claimed more than once, that was the first heat map. And in fact, North Carolina turned out to be the poster child of the area where the counties had the most claims from multiple cancer centers.”
Knudsen expects the initiative to generate a report that would “inventory” cancer disparities across the continent.
“I think we will find a lot of value in that,” Knudsen said. “So, we’re not just saying, ‘In Philadelphia County, here’s the issue,’ but ‘In 400 counties across the United States, here’s an issue,’ becomes a much more empowering message.”
Lerman’s two-year plan to create a diverse leadership pipeline would culminate in two deliverables: an AACI Leadership Development Workshop and an AACI Leadership Development Toolkit. Both programs are anticipated to include curriculums that would help new cancer center directors transition into their jobs and provide emerging leaders with the skills needed to navigate their careers.
Considering our data, you see that even at the research program leader level in the cancer centers, the associate directors level, if we started there, we’d still be working with a talent pool that’s not especially diverse as shown by the AACI data.
Caryn Lerman
“There was almost universal interest in participating in a program if offered by the AACI,” Lerman said at the meeting. “Components of such a program deemed by our centers to be most important include communication and collaboration, followed by skills development and career counseling to become a cancer center leader, as well as resiliency and negotiation skills.
“After badgering those centers who didn’t respond to the survey, we’ll more fully analyze the data and prepare a publication that also includes best practices for building, onboarding, and developing a diverse pipeline of cancer center leaders.”
Lerman’s and Knudsen’s presidential initiatives would, as one might say, kill two birds with one stone—creating a pipeline of diverse leaders with the skills and cultural competency to design targeted programs, based on the collected data, to effectively reduce cancer disparities at a hyperlocal scale.
“Through our collaboration on these AACI presidential initiatives, we aim to empower a diverse group of emerging leaders to take action to address the cancer disparities within the multicultural catchment areas they serve,’ Lerman said to The Cancer Letter.
Lerman’s remarks at the virtual AACI annual meeting follow:
Welcome. I’m Caryn Lerman, AACI president since July 2021, and director of the University of Southern California Norris Comprehensive Cancer Center. I’m delighted to share this presidential initiative with you today and look forward to your feedback.
The problem we’re trying to solve with this initiative is the disconnect between the capacity and diversity of the current cancer center workforce and the needs of our increasingly complex cancer centers.
The practice of oncology is evolving rapidly with new informatics technologies and precision therapies, while shifting reimbursement policies are affecting our cancer service line margins. Leadership skills are generally not taught during traditional clinical or biomedical training. And today’s leaders were often selected based on their excellence as clinicians, researchers, or educators.
Moreover, there’s a disconnect between our nation’s diversity and the diversity of the cancer center leadership workforce.
Closing this gap requires many factors, including but not limited to building a diverse pipeline from both within and outside of the center, implementing deliberate and tailored leadership development to build the skills necessary to succeed in a complex cancer center environment, and ensuring that our centers provide comprehensive onboarding and mentoring for new and emerging cancer center leaders.

To examine the potential for a presidential initiative in this area, and to define the scope and desired outcomes, I’m fortunate to collaborate with an exceptional team of center directors, associate directors and leaders in diversity, equity, and inclusion who formed this steering committee. This presentation is a product of our collaboration.

To establish a baseline for our initiative, we launched a survey that 59 of the AACI cancer centers have completed to date. For those of you who have not completed the survey, we will be sending another notice after the annual meeting. Those centers participating will be listed in the appendix of a publication to be developed from these data.
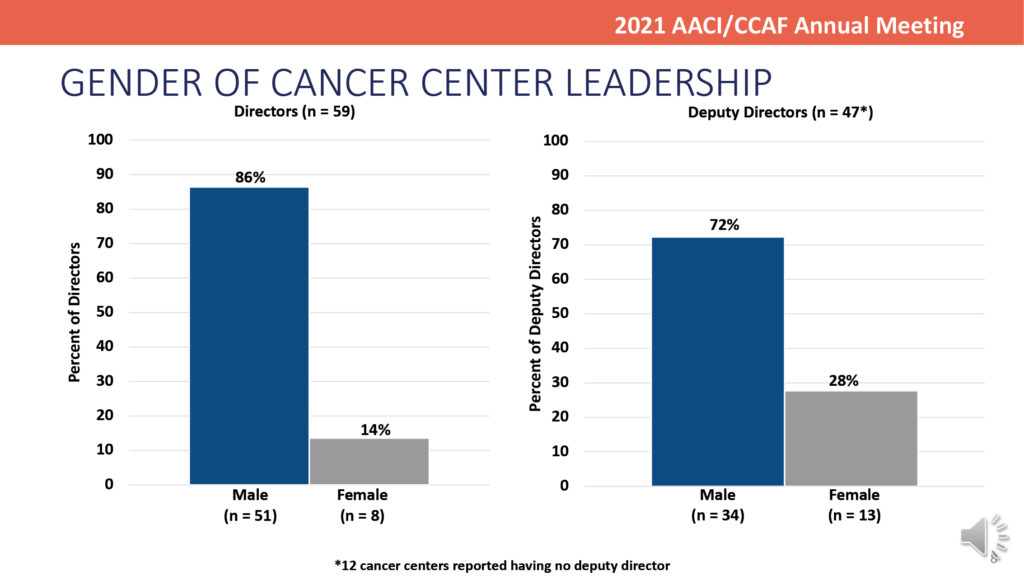
Our first goal was to characterize the race, ethnicity and gender of cancer center senior leaders at our centers to establish a baseline. As shown here, of the 59 respondents, the vast majority of our cancer center directors and deputy directors are non-Hispanic, white, and it’s not a big surprise, but they’re also predominantly male cancer center directors and deputy directors.

We also see this at the level of associate directors and research program leaders, suggesting that our pipeline of future leaders also lacks diversity. We start to get a bit closer for the gender of associate directors and research program leaders, though there are still opportunities for greater balance.

Assessing practices for building a diverse pipeline, our survey also shows that most centers use a combination of internal and external search practices, though making appointments without an internal-external search is still a fairly common practice, and one that can lead to appointments of the so-called usual suspects.

Strategies found to be most helpful in creating a diverse pool for senior leadership recruitments include the use of search firms, targeted placement of advertisements, and input from other leaders.

The majority of centers responding to the survey do not offer leadership development training programs at their centers, but there was almost universal interest in participating in a program if offered by the AACI.

Components of such a program deemed by our centers to be most important include communication and collaboration, followed by skills development and career counseling to become a cancer center leader, as well as resiliency and negotiation skills. Based in part on these data, our steering committees developed a set of deliverables and a rough timeline shown here.
After badgering those centers who didn’t respond to the survey, we’ll more fully analyze the data and prepare a publication that also includes best practices for building, onboarding, and developing a diverse pipeline of cancer center leaders.

This will lay the foundation for the development of curriculum to foster the onboarding of new cancer center directors and administrators, including such topics as cancer service lines, fund flow models, business acumen and others, and as well as a peer mentoring program. We will also develop a rotating career development curriculum for emerging leaders, emphasizing key skills for future development.
This will culminate in the first AACI leadership development workshop at the 2022 meeting with emphasis on underrepresented groups, followed by the creation of a toolkit for those centers that are interested in adapting the program and offering the program at their own institutions.
I look forward to your questions and feedback.
This story is part of a reporting fellowship on health care performance sponsored by the Association of Health Care Journalists and supported by The Commonwealth Fund.






